
Building a hospital is a monumental task, and the most critical work happens long before the first shovel hits the dirt. This initial strategic planning phase, which includes a deep-dive feasibility study, thorough market analysis, and meticulous space programming, is where the project's success is truly decided.
Get this part right, and you set the stage for a facility that meets clinical demands and financial targets. Skimp on it, and you're paving the way for costly rework and operational headaches down the line.
Building the Foundation Before Breaking Ground
The fate of a hospital project is sealed in its early planning. A rushed pre-design phase is a classic recipe for budget blowouts, inefficient workflows, and a building that just doesn't serve the community it was meant for. I like to think of this stage as mapping the hospital's strategic DNA—every decision made here will ripple through the entire design and construction process.
This foundational work ensures the building is a direct response to hard data, not just gut feelings or assumptions. For any developer or owner, this is your single most powerful tool for mitigating risk.
Getting the Market Analysis Right
Before a single blueprint is sketched, you have to know your market inside and out. A proper market analysis digs into the specific healthcare needs of the community you plan to serve. It's about finding out which service lines are desperately needed and which are already well-covered. This goes way beyond simple demographics; we’re talking about a forensic look at competitor services, local health trends, and even the dominant insurance providers in the area.
For example, your analysis might uncover an aging population with a high rate of heart disease but no dedicated cardiac center for miles. That’s a clear signal to prioritize a top-notch cardiology department, complete with cath labs and a cardiac ICU. On the flip side, it might show the area is saturated with maternity wards, steering you away from that investment.
You need to be evaluating data points like:
- Demographic Trends: Look at age, income, and population growth projections. This helps you see where the demand will be in 5, 10, or 20 years.
- Competitor Analysis: Literally map out who is doing what. Where are the gaps in care that you can strategically fill?
- Community Health Needs Assessment (CHNA): Public health data is a goldmine. It tells you the most prevalent diseases and health issues your future patients are facing.
This data-first approach shifts the project from a speculative venture to a strategic one. It ensures you’re not just building a hospital correctly, but that you’re building the correct hospital for that specific market.
The process flows logically from understanding the market to defining the space, and finally, to picking the right spot.
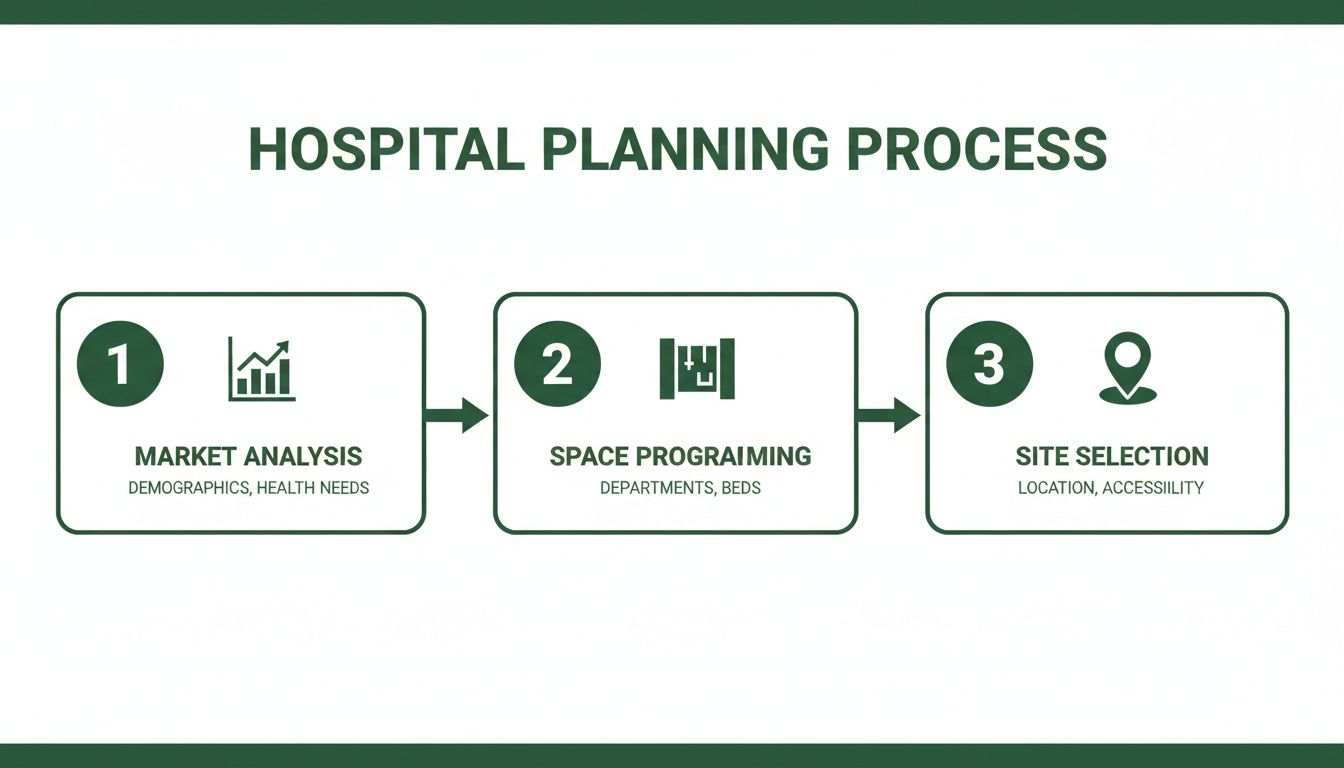
As you can see, each step builds on the last, creating a rock-solid plan for the entire project.
From Services to Square Feet: The Art of Space Programming
Once you know which clinical services you'll offer, the next job is space programming. This is where we translate those services into a highly detailed list of every single room, its required size, and how it needs to relate to adjacent spaces. Think of it as the project's architectural brief—a document that quantifies the entire facility, foot by foot. You simply can't build a functional hospital without it.
A detailed space program is the bridge between your strategic vision and the physical design. It puts numbers to the hospital's operational needs, giving the architect a precise roadmap and preventing the kind of scope creep that kills budgets and timelines.
Let’s take an emergency department. A program won’t just have a line item for "ED." It will break it down into the exact number of trauma bays, triage rooms, and standard exam rooms. It will specify support spaces like nurse stations, medication rooms, and decontamination showers. This painstaking detail is what creates a department that can handle a crisis smoothly, rather than descending into chaos. It's the difference between a building that fights your staff and one that works for them.
Navigating the Labyrinth of Healthcare Codes

Designing a hospital isn't just about architecture; it's about navigating a thicket of regulations. One wrong turn can lead to brutal delays and redesigns that blow up your budget. This isn't a simple box-ticking exercise. Getting it right means truly understanding the web of codes governing everything from how wide a corridor needs to be to the specifics of air filtration in an operating room.
Think of it as a layered puzzle. You have national standards, state-specific health department rules, and local zoning ordinances all piled on top of each other. They don't always play nicely together, and the real skill is in figuring out how to satisfy all of them from the very start.
The Key Players in Regulation
You’ll be answering to several different governing bodies, and each has its own rulebook and enforcement style. The Facility Guidelines Institute (FGI) is the big one, providing the foundational standards for most healthcare facilities across the U.S. Their guidelines are your starting point for patient room sizes, surgical suite layouts, and more.
But FGI is just the beginning of the story. Your state’s Department of Health will have its own licensing requirements that often add to or tweak the FGI standards. Then, local municipalities layer on their own building, fire, and zoning codes. It's a classic multi-jurisdictional headache.
The single biggest mistake a development team can make is assuming one codebook covers it all. You have to meticulously cross-reference state health mandates, FGI guidelines, and local ordinances to build a single, bulletproof compliance strategy.
For example, FGI might set a minimum for air changes per hour in an OR. Your state could demand a higher standard or specific filtration levels. Then, the local fire marshal will dictate the sprinkler systems and escape routes for that same room. You have to hit all three targets.
Common Hurdles and How to Clear Them
Some areas of hospital design are just magnets for compliance issues. Fire and life safety regulations are notoriously complex because the rules shift based on how a space is used. The requirements for an inpatient wing, an outpatient clinic, and a business office in the same building are all wildly different.
Ventilation is another minefield. Operating rooms, isolation rooms, and labs have incredibly strict rules for air pressure, filtration, and circulation to stop infections from spreading. These systems can't be an afterthought; they have to be baked into the architectural and structural plans from day one.
It’s also critical to get the electrical safety regulations right. For instance, knowing the ins and outs of the NEC tap rule for safe electrical wiring is essential for ensuring your power distribution systems are safe, compliant, and reliable.
Keep a close eye on these common trouble spots:
- Hazardous Materials: The rules for storing and handling medical gases, chemicals, and radioactive materials are unforgivingly precise.
- Accessibility: Meeting basic ADA standards is the floor, not the ceiling. Genuinely accessible design anticipates the needs of patients with a wide range of mobility challenges.
- Medical Equipment: Heavy-duty imaging equipment like MRIs and CT scanners needs serious structural, electrical, and plumbing support that must be planned for well in advance.
Working with the Authorities Having Jurisdiction
The best way to manage all this complexity is to stop thinking of regulators as adversaries. The Authorities Having Jurisdiction (AHJs)—the state and local officials who sign off on your plans—should be your partners.
Get them involved early. Schedule preliminary review meetings during the schematic design phase. Walk them through your approach and ask for their interpretation of any gray areas in the code. This kind of open communication can spot a problem months before it becomes a change order during construction. A good relationship built on transparency is your most valuable asset for a smooth approvals process.
2. Designing Clinical Spaces for Peak Performance
Let's get to the heart of the matter: the clinical core. This is where the life-and-death decisions happen, and the physical design of these spaces has a direct, measurable impact on patient outcomes and staff efficiency. It's not just about aesthetics. A poorly planned clinical area creates constant friction, leading to medical errors and burnout. A thoughtfully designed space, on the other hand, becomes a silent partner in delivering exceptional care.
We're going to walk through four critical zones: the Emergency Department (ED), Operating Rooms (ORs), Imaging Suites, and Inpatient Units. Each has its own rhythm and unique demands, but they all share a fundamental need for clear circulation, smart adjacencies, and layouts that actually support the complex work happening within them.
The Modern Emergency Department
Most people think of the ED as the hospital's "front door," but from a design perspective, it's more like a high-stakes sorting facility running 24/7 under immense pressure. One of the most effective strategies I’ve seen is creating completely separate entrances for walk-in patients and ambulance arrivals. It's a simple move, but it immediately de-escalates chaos, allowing staff to triage less urgent cases without being swamped by critical emergencies rolling in.
Inside, the best EDs are broken down into distinct zones or "pods" based on patient acuity. You'll have dedicated areas for trauma, acute care, and a "fast-track" for minor issues. This model creates parallel workflows, allowing for more focused staffing and preventing a patient with a sprained ankle from tying up a bed needed for someone having a heart attack. It’s all about managing the inherent unpredictability of emergency medicine.
Optimizing the Surgical Suite
When you step into the world of operating rooms, sterility is king. The design absolutely must create an uncompromising barrier between clean and dirty pathways. A time-tested and highly effective layout is the sterile corridor system. It's a one-way street: sterile supplies and surgical teams enter the OR from a clean side, while all soiled materials and post-op patients exit through a separate, non-sterile corridor on the other.
This one-way flow is the bedrock of infection control. It also forces careful planning of all support spaces. For example, the Sterile Processing Department (SPD)—where every instrument is meticulously cleaned and sterilized—needs a direct, secure connection to that sterile core to maintain the integrity of the whole system.
The physical layout of a surgical suite is a direct expression of its infection control philosophy. Designing for a clear separation between sterile and non-sterile zones isn't a recommendation; it's a fundamental requirement for patient safety.
The Rise of Outpatient Services
One of the biggest shifts shaping hospital design right now is the massive migration from inpatient to outpatient care. So many procedures that once required an overnight stay are now done on a same-day basis, and this has profound implications for how we plan and allocate space.
This shift is a dominant force in healthcare architecture. In fact, for many health systems, outpatient revenue now equals or even exceeds inpatient revenue. This reality is forcing a total reconfiguration of facilities to better support same-day surgery, infusion centers, and advanced imaging. We're seeing new hospital projects reduce dedicated inpatient beds by 10–30% compared to older facilities, while dramatically increasing the number of procedure bays and observation areas. For a deeper look into this industry-wide trend, check out SmithGroup's detailed health forecast.
What does this mean for design? Flexibility is everything. A pre-op bay might need to function as a post-anesthesia care unit (PACU) during peak hours. Rooms have to be adaptable, capable of handling different procedures without a major overhaul. That requires building in robust infrastructure from day one—more medical gas outlets, more data ports, and flexible power options are non-negotiable.
Designing Patient-Centered Inpatient Units
After a procedure, the inpatient unit is where recovery begins. Modern design has thankfully moved away from those long, sterile institutional corridors. The focus now is on more manageable, human-scaled layouts. A popular and effective model is the decentralized nurse station, which places smaller work areas directly between small groups of rooms.
This simple change brings nurses physically closer to their patients, cutting down on wasted steps and improving direct observation. It also fosters a much quieter, calmer environment by breaking up the constant hustle of a large, central station.
Other key features we always build into our inpatient unit designs include:
- Family Zones: Carving out dedicated space in the patient room for family members to sit, work, or rest comfortably. They are part of the care team.
- Same-Handed Rooms: This is a big one. We design all rooms with the exact same layout—bed on the left, bathroom on the right, for example. This standardization dramatically reduces the risk of medical errors because staff instinctively know where to find everything, especially in a code-blue emergency.
- Views and Natural Light: It's not a "nice-to-have." Ample windows with views of nature have been clinically shown to speed recovery times and lower stress. Orienting rooms to maximize daylight is a simple but powerful tool in the healing process.
Ultimately, designing a hospital’s clinical core is like solving a massive, three-dimensional puzzle of adjacencies, workflows, and future-proofing. When you get it right, you create an environment where caregivers can perform at their best and patients can heal in safety and comfort.
A critical piece of that puzzle is getting the departmental adjacencies right from the start. Placing departments that work together frequently next to each other saves precious time in transporting patients and equipment, which can be life-saving in an emergency.
Here's a look at some of the most critical adjacency pairings we prioritize in our planning.
Clinical Adjacency Planning Priorities
| Primary Department | High-Priority Adjacency | Rationale for Proximity |
|---|---|---|
| Emergency Department (ED) | Imaging (CT, X-ray), Lab Services | Immediate access to diagnostic tools is crucial for rapid triage and treatment of trauma and acute cases. |
| Operating Rooms (OR) | Sterile Processing (SPD), PACU | Ensures a sterile instrument supply chain and facilitates smooth, safe patient transfer before and after surgery. |
| Intensive Care Unit (ICU) | Surgical Suite, ED | Allows for quick transfer of critically ill patients from surgery or emergency intake to intensive monitoring and care. |
| Labor & Delivery | Neonatal ICU (NICU), OR | Co-locating these services provides immediate access to specialized care for high-risk newborns and emergency C-sections. |
| Cardiology | Catheterization Lab, Imaging (MRI/CT) | Streamlines the diagnostic-to-treatment pathway for cardiac patients, reducing transport time during critical events. |
| Oncology/Infusion | Pharmacy, Laboratory | Close proximity to the pharmacy is essential for the timely and safe preparation of chemotherapy drugs. |
Thinking through these connections early in the schematic design phase prevents major workflow headaches and operational inefficiencies down the road. It’s about designing for movement and logic, not just for static rooms on a floor plan.
Engineering for Safety and Long-Term Value

Great architecture and smart clinical layouts get a lot of attention, but a hospital’s real guts—its resilience and safety—are engineered deep within the walls. The mechanical, electrical, and plumbing (MEP) systems are the facility's lifeblood. This complex network is what truly dictates everything from patient recovery rates to the long-term operational budget.
For any developer or owner, making the right engineering calls upfront is one of the smartest ways to bake long-term value into the asset. We're not just talking about keeping the lights on. These systems are an active, critical part of the healing environment.
Mastering Air Quality for Infection Control
In a hospital, the air itself is a medical instrument. This is where Indoor Air Quality (IAQ) moves from a "nice-to-have" to a core design principle. Your HVAC system is the first line of defense against healthcare-associated infections (HAIs), which have devastating consequences for patients and providers alike.
The entire game is about precise control over air pressure, filtration, and circulation. For example, sensitive areas like operating rooms or protective units for immunocompromised patients must maintain positive air pressure. This means the pressure inside is slightly higher than outside, so when a door opens, clean, filtered air pushes out, keeping contaminants from drifting in.
On the other hand, airborne infection isolation rooms demand the opposite: negative air pressure. Here, the pressure is lower inside the room. This ensures that when the door is opened, any contaminated air is pulled into the room and safely exhausted, protecting the rest of the hospital. Pulling this off requires a meticulously balanced and sophisticated HVAC system.
The Role of Filtration and Air Changes
Filtration is another non-negotiable. And we’re not talking about the filters you buy at the hardware store. Healthcare facilities depend on High-Efficiency Particulate Air (HEPA) filters, which are engineered to capture 99.97% of airborne particles as small as 0.3 microns. They're absolutely essential in sterile environments for pulling bacteria, viruses, and other pathogens right out of the air.
Just as critical is the concept of Air Changes per Hour (ACH). This metric tells you how many times the entire volume of air in a room is swapped out with fresh, filtered air every hour. The demands vary dramatically by space:
- Standard Patient Rooms: Typically require a minimum of 6 ACH.
- Operating Rooms: Need a much higher rate, often 20 ACH or more, to quickly clear any contaminants.
- Isolation Rooms: Require at least 12 ACH to ensure effective containment and safety.
Thinking about MEP systems solely in terms of upfront cost is a critical mistake. These systems represent a massive portion of a hospital's long-term operational budget. Investing in high-efficiency equipment and smart design from day one is one of the most effective ways to reduce lifecycle costs and boost the asset's overall financial performance.
Building Resilient Infrastructure
Beyond air quality, a hospital's core infrastructure must be designed for absolute, bulletproof reliability. Failure is simply not an option. That means engineering for redundancy in every key system.
Take the medical gas system, for instance—the network that delivers oxygen, medical air, and vacuum to patient bedsides. It must have multiple backups and alarms that instantly alert staff to any pressure drops.
The same goes for emergency power. Hospitals are required to have backup generators powerful enough to run life-support systems, surgical suites, and critical monitoring equipment for an extended time during an outage.
Water is another weak point if not planned for. The design must include a strategy for maintaining a supply of potable water during a municipal service interruption, often through large on-site storage tanks. This is the kind of resilient infrastructure that allows a hospital to keep saving lives when external utilities go down.
Hospitals are notorious energy hogs, but that consumption also creates a huge opportunity. A 300,000-square-foot hospital that manages to cut its energy use by 40% could save anywhere from hundreds of thousands to over a million dollars a year. This makes investing in high-efficiency systems a powerful financial move, not just an environmental one.
Adaptive reuse strategies, like those we champion at Sherer Architects, can push sustainability even further by extending a building's life and cutting embodied carbon by up to 20-40% versus new construction. You can dig deeper into these trends in the 2025 Hospital Construction Survey.
Getting the Project Built: Delivery Models and Financial Planning

This is where the rubber meets the road. All the meticulous planning and brilliant design in the world won't matter if the project stumbles on a shaky financial foundation or gets bogged down by the wrong delivery method. For developers and owners, turning that vision into a physical, functioning hospital boils down to mastering the numbers and the team structure.
An elegant design is just a pretty picture if the budget is a fantasy or the delivery model creates conflict instead of collaboration. This phase is all about managing risk and making smart decisions that safeguard your investment for decades to come.
Building a Bulletproof Hospital Budget
A hospital budget is a different beast entirely from other commercial projects. The complexity is immense, and it’s easy to get fixated on the obvious hard costs—the concrete, steel, and labor—and completely underestimate everything else.
The real budget-busters are often hiding in the soft costs. From my experience, these can easily swell to 25-35% of your total project cost. If you don't account for them accurately from the very beginning, you’re setting yourself up for a world of financial pain down the line.
A truly comprehensive budget has to cover a lot of ground:
- Professional Fees: This isn't just the architect and primary engineers. Think about the army of specialty consultants you'll need: medical equipment planners, acousticians, IT infrastructure experts, and more.
- Permitting and Approvals: The fees and time required to navigate state health departments and local jurisdictions are significant. Don't treat this as an afterthought.
- Medical Equipment (FF&E): Furniture, fixtures, and especially the high-tech medical equipment are a massive capital line item. We're talking about everything from hundreds of patient beds to multi-million-dollar MRI and CT scanners.
- Contingency Funds: This is non-negotiable. A healthy contingency, typically in the range of 5-10% of total construction costs, is your safety net for the inevitable surprises and changes that pop up during construction.
Choosing the Right Project Delivery Model
How you structure the relationship between the owner, designer, and contractor will fundamentally shape your project's outcome. The old-school Design-Bid-Build approach, where you finish the design completely before hiring a contractor, is often slow and can create an adversarial "us vs. them" dynamic.
In the world of complex healthcare projects, more collaborative models are quickly becoming the standard. They just make more sense. Bringing everyone to the table early aligns goals and fosters a problem-solving mindset from day one.
The delivery model you choose is a strategic decision that shapes the entire project dynamic. For a complex build like a hospital, collaborative models that bring the contractor on board early are almost always superior for managing costs, schedule, and risk.
Let's look at two of the most effective alternatives:
- Design-Build: Here, you sign a single contract with one entity that handles both design and construction. This single point of responsibility is a game-changer. It streamlines communication, slashes change orders, and can seriously compress the project timeline.
- Integrated Project Delivery (IPD): This is the ultimate team sport. The owner, architect, and contractor all sign a multi-party agreement, sharing both the risks and the rewards. IPD drives incredible transparency and teamwork, making it perfect for the most complex or fast-tracked hospital projects.
The trend is undeniable. The U.S. hospital construction market, which hit an estimated $34.6 billion in 2025, is heavily shifting toward these collaborative methods. In fact, industry analysis suggests that design-build will account for about 47% of construction spending by 2028, largely because it can accelerate project delivery by 10–25%. If you want to dig deeper into these trends, you can find additional hospital construction insights on ibisworld.com.
The Financial Case for Resilience
A smart financial plan doesn't just stop on opening day. It has to look decades into the future and account for the hospital's long-term resilience. A facility that can’t keep its doors open during a hurricane, power grid failure, or the next pandemic is a fragile and deeply flawed asset.
Investing in resilience means hardening your facility against predictable threats. This could mean elevating critical MEP equipment above the flood plain, engineering the structure for higher wind loads, or building robust on-site power generation and water reserves.
Yes, these measures can add 5–15% to the initial construction cost. But the ROI is crystal clear. You're buying an insurance policy against catastrophic operational downtime and the staggering financial losses that follow. It’s an investment that protects revenue, staff, and the community when disaster strikes, ensuring your hospital can fulfill its core mission no matter what.
Common Questions About Designing a Hospital
Diving into a hospital project for the first time? It's natural to have questions. In my experience, a few key queries always seem to pop up early on. Let's tackle them head-on, so you can move forward with a clearer picture.
How Long Does The Hospital Design Process Typically Take?
You're looking at a design phase of roughly 12 to 24 months from the very first programming meeting until you have a set of construction-ready documents in hand. Of course, that's a wide range, and the final timeline really depends on the hospital's size, complexity, and how many specialty services you plan to include.
This period breaks down into the usual stages: schematic design, design development, and finally, the nitty-gritty construction documents. But it's the external factors that often stretch the schedule. Things like state regulatory reviews or navigating a tricky Certificate of Need (CON) process can easily tack on several extra months.
One way to potentially tighten this up is with a more integrated project delivery method. A design-build approach, for instance, can let design and early construction phases overlap, shaving valuable time off the total project duration.
What Is The Biggest Design Mistake To Avoid?
Hands down, the costliest and most frequent error I see is rushing the pre-design planning.
When a team jumps into schematic design without a solid, rigorously vetted space program and a real understanding of clinical workflows, it's a recipe for disaster. Why? Because every single change order made during construction is exponentially more expensive than a change made on paper.
Another common blind spot is failing to grasp the sheer volume required for all the MEP (mechanical, electrical, plumbing) systems. These aren't just pipes and wires; they are the hospital's lifeblood and can easily eat up 25-30% of the building's total volume. If you don't account for that massive footprint from day one, you’ll find yourself in a constant battle for space, forcing costly architectural compromises down the line.
Insufficient pre-design planning is the single most reliable predictor of budget overruns and operational headaches. The time and resources invested in meticulous upfront programming will pay for themselves many times over throughout the project's life.
How Can We Future-Proof A New Hospital Design?
Future-proofing isn't about predicting the future; it's about designing for flexibility. Healthcare delivery is always evolving, technology gets upgraded, and patient demographics shift. A smart building needs to adapt without requiring a complete teardown and rebuild.
Here are a few strategies we always build into our projects:
- Embrace Modular and Universal Designs: By creating standardized room layouts, you build in agility. An exam room can be converted into a consultation space, or an office can become a small treatment room with minimal fuss.
- Plan with "Soft Space": This is a simple but powerful concept. We deliberately place areas with simpler infrastructure—like administrative offices—right next to high-revenue clinical zones. When it's time to expand your OR suite or imaging department, you're knocking down drywall, not relocating major plumbing stacks.
- Oversize Your Core Infrastructure: It’s far cheaper to build in extra capacity now than to add it later. Designing your MEP, IT, and structural systems to handle future technologies and higher patient loads gives you room to grow without a massive capital expense.
What Role Does Adaptive Reuse Play In Healthcare Development?
Adaptive reuse has become an incredibly important tool for health systems. It's a smart way to expand services quickly and manage costs. We're seeing more and more clients convert existing structures, like old office buildings or even big-box retail centers, into outpatient clinics, ambulatory surgery centers, or specialty care facilities.
The big win here is speed. It's almost always faster than ground-up construction.
But the benefits don't stop there. This approach is also inherently more sustainable. You reduce embodied carbon by keeping the original structure, you minimize demolition waste, and you can significantly lower the initial capital investment. For a healthcare provider, it's a powerful way to establish a footprint in a new community while breathing new life into an existing building.
The journey from an idea to a fully functioning hospital is incredibly complex. But with the right architectural partner, it can be a smooth and profitable one. At Sherer Architects, LLC, we specialize in guiding owners through every stage of commercial design, adaptive reuse, and historic preservation. We're here to help you solve the puzzle, aligning every piece to deliver a beautiful, enduring, and successful project. Learn how we can bring structure to your vision at https://shererarch.com.