When you talk about the architecture of a hospital, you’re not just talking about putting up a building. You’re talking about crafting a dynamic, living ecosystem that’s engineered from the ground up to promote healing. It’s a blueprint where clinical precision has to meet human compassion, and every single space, from a corridor to a patient room, plays a role in someone's recovery.
The Blueprint For Healing: Understanding Hospital Architecture

The best way to think about a modern hospital is as a "city within a city." This isn't just a clever phrase; it’s the key to understanding the sheer complexity involved. Every department—the emergency room, surgical suites, patient wards, the cafeteria—is like its own distinct neighborhood. Each has a specific function, a unique population, and its own set of needs.
And just like a real city, a hospital needs infrastructure to survive. It relies on a carefully planned network of corridors (the streets), specialized MEP (Mechanical, Electrical, and Plumbing) systems (the utilities), and shared resources. The success of this entire "city" hinges on how well these different neighborhoods connect and support each other.
More Than Just Rooms and Hallways
A poorly designed hospital creates constant, daily friction. It's like a city where the fire station is miles from the main business district, or the grocery stores are nowhere near the residential areas. In a hospital setting, that translates into life-threatening delays in care, staff burning out from walking miles every shift, and an incredibly stressful environment for patients and their families.
The real craft of hospital architecture is in preventing these problems by focusing on a few core principles:
- Logical Adjacency: This means putting related departments right next to each other. Think imaging right beside the ER. It’s a simple concept that shaves critical minutes off travel time for patients and staff.
- Clear Circulation: You need separate, intuitive pathways for patients, staff, and supplies. This isn't just for efficiency; it’s a critical measure to prevent cross-contamination and operational gridlock.
- Patient-Centered Spaces: Designing rooms and waiting areas that actually make people feel better is non-negotiable. We're talking about reducing anxiety, providing comfort, and maximizing natural light, which is proven to speed up recovery.
- Operational Efficiency: Support services—the labs, pharmacies, and sterilization facilities—need to be centrally located so they can effectively serve every single department without becoming a bottleneck.
The Impact of Thoughtful Design
The architecture of a hospital directly impacts its viability for decades to come. When you’re developing the blueprint for a healing environment, every detail has consequences. For example, a detailed guide on choosing healthcare furniture for modern facilities is an essential piece of the puzzle, influencing everything from patient comfort to staff workflow.
A well-designed hospital is a strategic asset. It not only improves patient outcomes but also enhances staff retention, reduces operational costs, and strengthens the facility's reputation within the community.
Ultimately, the goal is to create a building that actively participates in the healing process. For developers and owners, grasping this is what separates a standard construction project from the creation of a vital community anchor—a place where good design literally saves time, money, and lives.
Choosing The Right Model: Hospital Typologies Explained
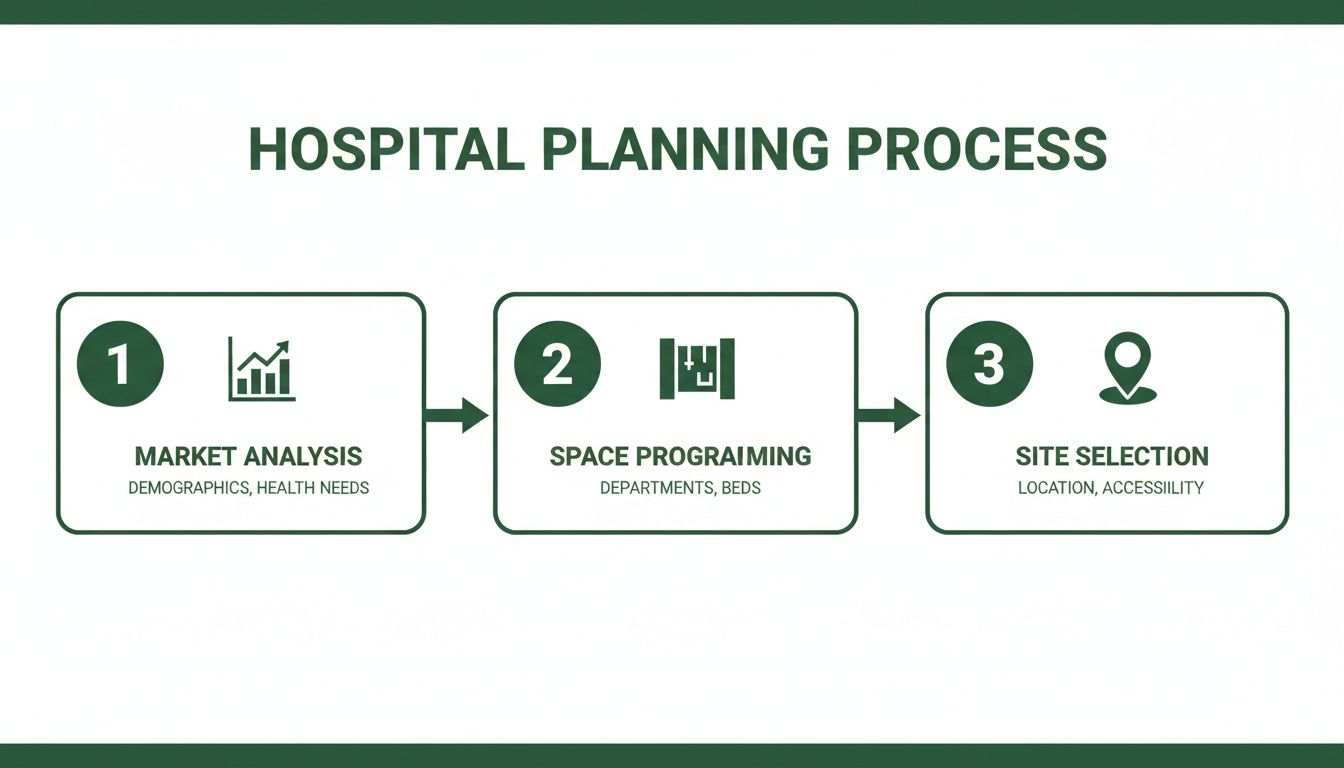
When you're at the very beginning of a hospital project, one of the first big decisions on the table is the foundational layout, or what we in the industry call the typology. This isn't just an aesthetic choice; it's a strategic move that sets the stage for everything that follows—from how much land you'll need and how the budget gets allocated to how easily the facility can grow and how smoothly it runs day-to-day.
Think of it like this: are you building a skyscraper, a sprawling suburban subdivision, or a town center? Each has a completely different footprint and serves a unique purpose. The same logic applies to hospitals.
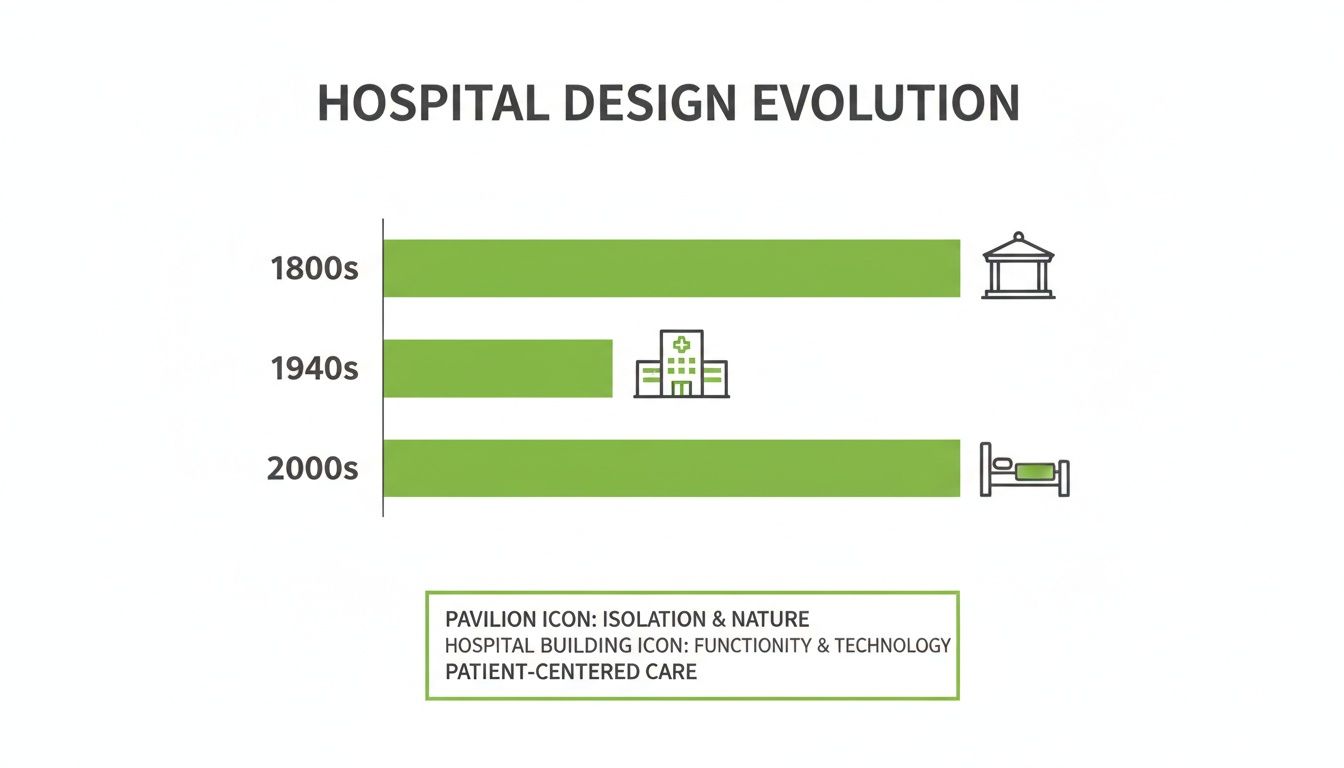
The models we use today really started taking shape in the 1960s. As medicine became more specialized, the design of hospitals had to follow suit. The old, monolithic do-it-all buildings gave way to campuses with distinct, free-standing structures, each dedicated to a specific function. If you're interested, you can learn more about how specialization reshaped healthcare design in the 1960s.
The Vertical Tower Model
The vertical tower is exactly what it sounds like: the high-rise of the hospital world. In this model, we stack departments one on top of the other in a compact, multi-story building. It's the go-to solution for tight urban sites where every square foot of land comes at a premium.
The biggest win here is efficiency on a small footprint. You can pack a full-service medical center onto just a couple of acres by building up, not out. This approach also centralizes the building's guts—elevators and core MEP (Mechanical, Electrical, and Plumbing) systems—which can make logistics feel a lot simpler. But that compactness has its trade-offs. The entire building lives and dies by its elevators, which can easily become bottlenecks for moving patients, staff, and supplies.
The Horizontal Campus Model
On the complete opposite end of the spectrum is the horizontal campus. This model feels more like a small village or a low-rise corporate park, spreading departments out across a large piece of land in a series of interconnected, one or two-story buildings. It’s a natural fit for suburban or rural areas where land is abundant and affordable.
The real beauty of the campus model is its built-in flexibility for phased construction and future growth. Adding a new wing or even an entirely new building is far more straightforward than trying to tack another floor onto a tower. These layouts also tend to feel less institutional and more calming, with plenty of opportunities for green spaces and courtyards. The major drawback? The sheer distances people have to cover. Staff and patients might face long walks between departments, which can affect everything from emergency response times to simple navigation.
A key consideration for developers is that the chosen typology directly impacts long-term flexibility. A horizontal campus offers modular growth, while a vertical tower locks in a more rigid structure, making future adaptation more complex and costly.
The Hybrid Model
The hybrid model is an attempt to get the best of both worlds. It usually involves a central, multi-story tower for acute care services—think surgery and the ICU—which is then connected to lower-rise wings that house outpatient clinics, administrative offices, and diagnostic centers. This blended approach is getting more and more popular because it strikes a great balance between density and flexibility.
With this setup, you can centralize the critical, high-traffic departments vertically for peak efficiency while letting less urgent services spread out horizontally. It creates a natural, logical separation between inpatient and outpatient traffic, which makes the experience better for everyone. By pairing a dense core with expandable outer buildings, the hybrid model gives owners a practical design that can actually adapt as healthcare needs change over time.
Comparing Hospital Architectural Models
To see how these models stack up against one another, it helps to put their core features side-by-side. This table breaks down the key characteristics of each typology to help developers get a clearer picture of what might work best for their specific site and long-term vision.
| Model Type | Key Characteristic | Best For | Primary Challenge |
|---|---|---|---|
| Vertical Tower | A compact, multi-story high-rise with stacked departments. | Dense urban areas with limited land availability. | Reliance on elevators and limited options for future expansion. |
| Horizontal Campus | A sprawling, low-rise layout with interconnected buildings. | Suburban or rural sites with ample land for growth. | Long travel distances between departments and potential wayfinding issues. |
| Hybrid Model | A central tower connected to lower-profile outpatient wings. | Sites that need to balance density with future flexibility. | Requires careful master planning to ensure seamless integration. |
Ultimately, there's no single "right" answer. The best model depends entirely on the project's unique constraints and goals, from the available land and budget to the community it will serve and the vision for its future.
Designing for Seamless Patient and Staff Flow
Once you’ve settled on a hospital's big-picture model, the real work begins inside. We have to design the internal logic—that complex web of hallways, elevators, and rooms that dictates how everyone and everything moves through the space.
It’s a bit like designing a major airport terminal. The path for an international traveler heading through security and customs is completely different from someone being dropped off for a quick domestic flight. In the same way, the architecture of a hospital must create clear, efficient, and separate routes for patients, staff, and the public.
Get this wrong, and you get chaos. You’ll have crowded hallways where a patient on a gurney is trying to get past a food delivery cart while a lost family is looking for the cafeteria. This isn't just an annoyance; it’s a direct risk to patient safety, a huge source of stress for staff, and a major drain on efficiency. The goal is to design a building where movement is so logical it feels effortless.
Mapping the Patient Journey
To get there, architects start by mapping out what we call "patient journeys." Let’s take someone arriving at the emergency department (ED) with chest pain. A well-designed flow gets them from the ambulance bay to a trauma room, then to an adjacent imaging suite for a scan, and finally up to a cardiac cath lab or the intensive care unit (ICU).
Every single step in that journey demands immediate access to the next. This is why clinical adjacencies are one of the most critical rules in hospital design. Putting imaging services right next to the ED means you avoid long, risky trips down public hallways. Similarly, situating surgical suites close to the ICU ensures post-op patients get to critical care without delay.
The guiding principle is simple: shrink the distance and time for the most critical pathways. A layout that saves a nurse 30 steps every time they perform a task can add up to miles of walking over a single shift. That means less fatigue and more time spent on actual patient care.
This evolution in hospital models directly influences how these internal flows are designed.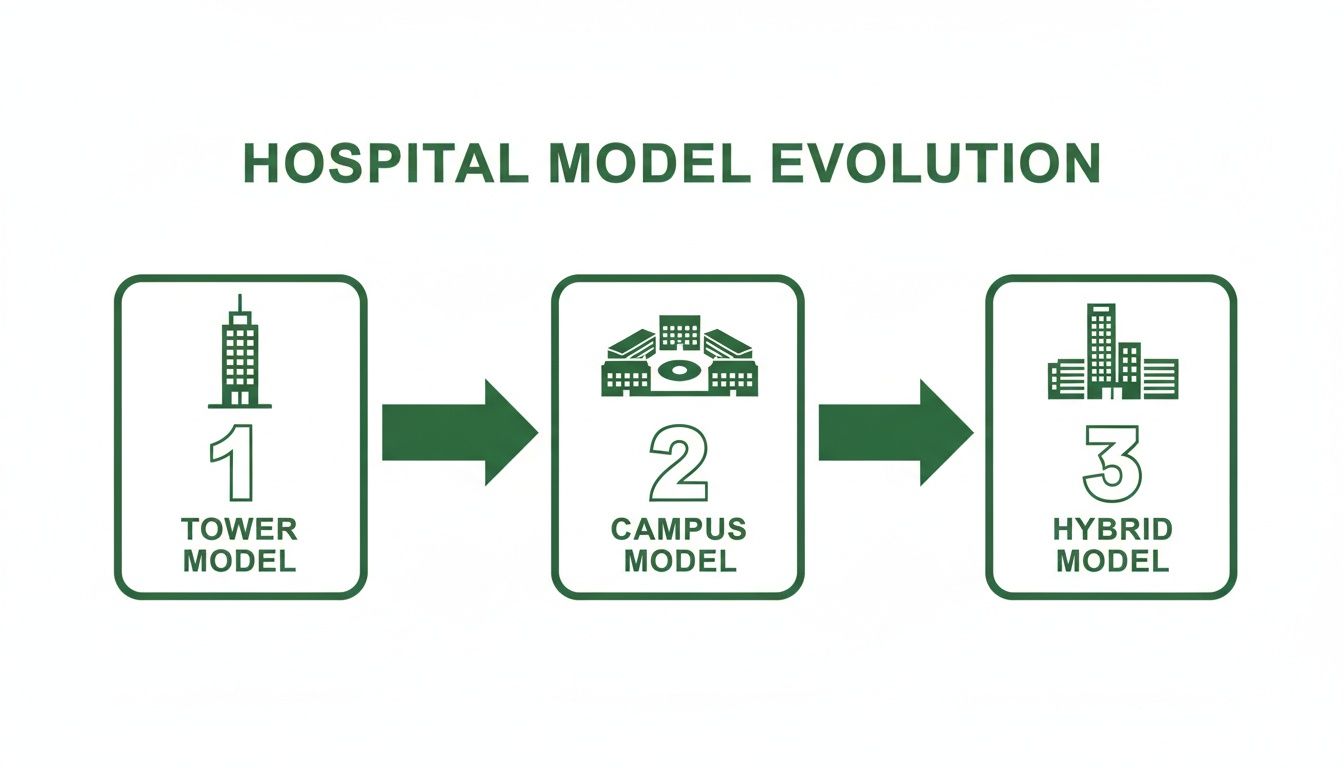
As you can see, each typology—from a dense vertical Tower to a sprawling Campus and a more balanced Hybrid—creates its own set of challenges and opportunities for laying out these vital patient and staff routes.
Separating "Onstage" and "Offstage" Traffic
Great hospital design also borrows a concept from the theater: separating the "onstage" action from the "offstage" work.
Public/Onstage Flow: Think of these as the main arteries—the lobbies, waiting rooms, and public corridors that patients and visitors use. They need to feel welcoming, be easy to navigate with clear signage, and be kept separate from the clinical and service hustle.
Staff/Offstage Flow: These are the dedicated, staff-only corridors and elevators. They’re the secret sauce that allows doctors and nurses to move quickly between departments without fighting public crowds. They also provide a clean route for moving sterile supplies and medication.
Service Flow: This is the circulation for things like food carts, linen services, and waste removal. These pathways have to be completely isolated from everything else to maintain hygiene and stop cross-contamination.
This onstage/offstage separation is fundamental. It prevents bottlenecks, keeps patient areas quieter, and protects the sterility of clinical zones. In the end, a hospital’s internal layout is the invisible force shaping its daily rhythm. When done right, it creates a calm, safe, and intuitive environment that leads to better patient outcomes, happier staff, and a far more successful healthcare facility.
The Hidden Infrastructure Of A Modern Hospital

Look past the patient rooms and surgical suites, and you'll find the true heart of a hospital: a massive, unseen network of critical systems. This is the building’s Mechanical, Electrical, and Plumbing (MEP) infrastructure. It's best to think of it as the facility's central nervous and circulatory systems combined—a complex web of pipes, wires, and ducts keeping everything alive and safe, 24/7.
These systems are anything but standard. A hospital's MEP infrastructure is built to support life-critical functions, often under extreme pressure. For any developer or owner, getting a handle on the sheer scale and cost of this hidden world is crucial. It can easily eat up a huge chunk of the construction budget and demands specialized expertise right from the start.
HVAC Systems That Do More Than Control Temperature
In a hospital, the Heating, Ventilation, and Air Conditioning (HVAC) system is a front-line defense in infection control. It's not just about keeping people comfortable. This system is engineered to maintain clinically mandated temperatures, humidity levels, and precise air change rates. Some areas, like isolation wings, may even require 100% fresh air intake with zero recirculation to stop airborne pathogens in their tracks.
These complex environmental controls are a core part of the hospital's infrastructure, and accurately projecting their cost is essential—often done using tools like Exayard HVAC estimating software. The system’s main job is creating specific pressure zones, which are absolutely non-negotiable for keeping patients safe.
Two great examples of this in action are:
- Negative Pressure Rooms: Built for patients with contagious airborne illnesses, these rooms constantly pull air in and filter it before sending it outside. This simple principle ensures infectious particles can't escape into the hallways.
- Positive Pressure Rooms: On the flip side, operating theaters and rooms for immunocompromised patients are pressurized to constantly push air out. This creates a sterile bubble, preventing contaminants from the surrounding areas from ever getting in.
The Unseen Lifelines: Medical Gas And Emergency Power
Tucked away inside the walls and ceilings is another lifeline: a dedicated network of pipelines delivering essential medical gases. These systems pipe oxygen, medical air, and vacuum suction directly to the bedside and into operating rooms. The codes governing their design are incredibly strict for one simple reason—failure is not an option.
Just as important is the electrical system’s resilience. A hospital simply has to stay running, even during a city-wide blackout. This demands a bulletproof emergency power setup, complete with massive generators and uninterruptible power supply (UPS) systems.
A hospital's emergency power system isn't just for the lights. It is legally required to support all life-sustaining equipment, from ventilators in the ICU to the surgical equipment in the operating room, without a moment's interruption.
Building in this level of redundancy is a major driver of cost and complexity. The electrical switchgear and generator plants required are massive, expensive, and need a significant amount of physical space planned into the building's footprint from day one.
Water Management And Specialized Plumbing
Finally, a hospital’s plumbing is worlds away from what you’d find in any other commercial building. It has to handle everything from the ultra-pure water required for labs and dialysis to the safe disposal of hazardous medical waste. These systems are designed with extensive backflow prevention to ensure there’s zero chance of cross-contamination between drinking water and waste streams.
Weaving all these intricate MEP systems together is a monumental challenge. It requires tight, constant coordination between architects, engineers, and contractors from the very first sketch. If you fail to plan for the spatial and structural needs of this hidden infrastructure, you’re setting yourself up for catastrophic budget overruns, crippling delays, and a final design that could compromise patient safety.
The Rules of the Game: Mastering Healthcare Codes and Regulations
Hospital architecture is a game played on a field defined by codes and standards. These aren't just bureaucratic red tape; they're the hard-won lessons from decades of medical practice, crystallized into rules that make healthcare facilities fundamentally safe, accessible, and ready for anything. For any owner or developer, getting a handle on this regulatory world isn't just a good idea—it's the only way to deliver a building that works.
Think of these regulations less as a checklist and more as the DNA of a successful hospital. They influence everything, from how wide a hallway needs to be for a gurney to pass a crash cart, to the specific fire-rating of a door separating an operating room from a corridor. Nail this from the beginning, and you avoid the nightmare of costly rework and delays in getting your doors open.
The Must-Know Codes and Standards
While the full library of codes can be intimidating, a few key documents are the foundation of nearly all hospital design in the U.S. The big one is the FGI Guidelines for Design and Construction. This is the go-to resource for minimum standards on everything from planning to building hospitals and clinics. It's so well-regarded that most states adopt it, either in full or with minor tweaks, as their legal standard.
Right alongside it is the Americans with Disabilities Act (ADA). This is non-negotiable. The ADA dictates that every corner of the facility—from the slope of the parking lot ramps to the height of a check-in counter and the layout of a patient bathroom—is usable by everyone. This isn't just about avoiding a lawsuit; it's about a core ethical commitment to providing equal access to care.
A rookie mistake is to treat code compliance like a final inspection item. The pros integrate these requirements into the schematic design from the very first meeting. Weaving FGI and ADA principles into the project from day one saves an incredible amount of time, money, and headaches later on.
Marrying Compliance with Green Building Goals
These days, smart design is all about hitting two targets with one stone: meeting strict regulatory demands while also pursuing ambitious sustainability goals. The good news is that these two objectives often go hand-in-hand. For example, modern energy codes practically demand the same high-performance building envelopes and efficient HVAC systems that are central to green building certifications like LEED.
This overlap creates a compelling financial argument for building green. A hospital designed for energy efficiency doesn't just shrink its carbon footprint; it also slashes its operating expenses for decades to come, which can mean millions in savings over the life of the building.
Here are a few practical examples of how this works:
- High-Performance Glazing: Installing advanced windows that block summer heat and retain winter warmth helps you meet tough new energy codes. It also makes patients more comfortable and takes a huge load off your HVAC system.
- LED Lighting and Controls: Shifting to smart lighting with occupancy sensors is a great way to meet energy efficiency requirements. The bonus? It can easily cut your lighting-related electricity costs by 50% or more.
- Water-Saving Fixtures: Specifying low-flow faucets and toilets is often required by modern plumbing codes, but it also directly cuts your facility's massive water and sewer bills.
- Durable, Healthy Materials: Choosing materials that are built to last and don't off-gas harmful chemicals (low-VOC) helps satisfy health and safety regulations while also improving indoor air quality—a huge win for both patients and green building credits.
In the end, navigating the web of healthcare regulations is about much more than just ticking boxes to avoid fines. It's a chance to build a smarter facility—one that's safer for patients, more functional for staff, and far cheaper to run. When you bake these requirements into the design from the start, you create a high-performing asset that will deliver value for years to come.
The Business Case For Hospital Development And Reuse
For any developer or property owner eyeing the healthcare space, one thing is clear: a hospital is as much a financial equation as it is a design marvel. You have to look past the blueprints and building codes to see the intricate business case—a delicate balance between massive upfront investment, long-term operational health, and profound community value.
Whether you're breaking ground on a new campus or breathing new life into an old building, the numbers are daunting. Hospitals are among the most expensive commercial projects to get built, largely because of the complex, often invisible infrastructure that makes them work. Specialized MEP (Mechanical, Electrical, and Plumbing) systems—think medical gas lines, redundant emergency power, and hospital-grade HVAC—chew up a huge slice of the budget.
These systems aren't optional extras; they're the lifeblood of the facility. They must be integrated perfectly from day one, which makes getting those estimates right early on absolutely crucial for keeping the project financially on track.
The Phasing Puzzle: Maintaining Operations During Construction
One of the biggest headaches in healthcare projects is trying to renovate or expand a hospital that can't simply close its doors. This is where a sharp project phasing strategy comes in. You have to break the entire construction process down into a series of manageable, carefully sequenced stages.
It’s a lot like performing surgery on the building itself. Every move has to be meticulously planned to cause the least possible disruption to patient care happening just a few feet away.
A typical phasing plan usually involves a few key steps:
- Decanting: This is the process of temporarily moving a whole department to another part of the hospital or even into a modular unit outside.
- Containment: We use heavy-duty physical barriers and negative air pressure systems to completely seal off construction zones. This is vital for controlling dust, noise, and vibration.
- Sequenced Handovers: Once a section is finished, it's fully commissioned and tested. Only then do we move staff and patients in before we even think about starting the next phase.
This approach keeps the hospital running, but there's no sugar-coating it—it adds significant time, complexity, and cost to the project.
The real art of phasing is creating a series of self-contained construction "bubbles" inside a living, breathing hospital. It allows the facility to continue its life-saving work uninterrupted while the building literally evolves around it.
The Value of Adaptive Reuse: A Sustainable Strategy
While starting with a clean slate is tempting, the adaptive reuse of existing buildings presents a really compelling business case. Turning an old office building, a warehouse, or a dated medical facility into a modern hospital can be a smarter, faster, and more sustainable path.
History gives us some great perspective here. Back in Renaissance Florence, a hospital building boom was directly linked to the city's explosive growth. As the population grew, these institutions transformed from simple shelters into wealthy, powerful anchors of the urban landscape. It’s a perfect example of the deep-rooted connection between healthcare infrastructure and a thriving community. You can dig deeper into this fascinating connection and the origins of hospital architecture.
Today, adaptive reuse is the modern version of that story. By giving an old building a new purpose, developers can meet today's medical needs while preserving a piece of the community's character. It's an approach that sidesteps the huge carbon footprint of demolition and new construction and often allows you to tap into existing infrastructure. For a developer, it's a chance to build a forward-thinking healthcare asset that's both a nod to the past and a very shrewd investment in the future.
Common Questions About Hospital Architecture
If you're a developer, investor, or property owner stepping into the world of healthcare projects, you've probably got a few questions. Hospital architecture is its own beast, and this section is here to give you straightforward, practical answers to what we hear most often.
How Long Does It Take to Design a Hospital?
There's no cookie-cutter answer, but for a typical mid-sized hospital, you should plan on 18 to 24 months just for the design phase. That's before a single shovel hits the dirt. This window covers everything from the initial programming and high-level master planning all the way down to the fine-grained construction documents.
Why so long? It's a massive coordination effort. Architects have to work hand-in-glove with specialized MEP engineers, get constant feedback from clinical teams who will actually use the space, and navigate a maze of regulatory approvals. Trying to shortcut this phase is a recipe for expensive change orders and frustrating delays during construction.
What's the Most Expensive Part of Building a Hospital?
While the concrete and steel are significant, the real budget-buster in hospital construction is almost always the Mechanical, Electrical, and Plumbing (MEP) systems. You can expect these complex networks to eat up anywhere from 30% to 50% of your total construction cost—a much bigger slice of the pie than in a standard office or retail building.
Several things drive this high price tag:
- Sophisticated HVAC: You're not just cooling a building. You're creating meticulously controlled environments, like negative-pressure rooms for infection control, which requires powerful and highly specialized air-handling equipment.
- Medical Gas Lines: Hospitals need a dedicated plumbing system for life-saving gases like oxygen, medical air, and vacuum. It's an essential, non-negotiable utility.
- Fail-Safe Power: When the power goes out, critical life-support machines can't. That means redundant generators and uninterruptible power supplies are an absolute must.
When you're putting together a pro forma for a hospital, seriously front-load the MEP budget. Underestimating this line item is one of the quickest ways for a healthcare development project to go off the rails financially.
Is It Better to Renovate an Old Hospital or Build a New One?
This is the million-dollar question, and the answer comes down to a tough cost-benefit analysis. On one hand, renovating an existing building—a form of adaptive reuse—can be cheaper and faster. If the building's structural "bones" are good, you get a huge head start. It's also a big win for sustainability, as you're saving tons of material from the landfill.
The catch is that older buildings often hide a hornet's nest of problems. Their infrastructure might be completely inadequate for today's high-tech medical equipment, or they might be a nightmare to bring up to current building codes. A new build, while more expensive upfront, gives you a blank canvas. You can design for perfect patient flow, seamlessly integrate the latest technology, and plan for future growth without being boxed in by an old layout. The best path forward really depends on the state of the old building, your site, the budget, and what you want the hospital to be in 10 or 20 years.
At Sherer Architects, LLC, we help owners and developers make these kinds of complex decisions every day. With our deep experience in commercial architecture, adaptive reuse, and historic preservation, we know how to transform challenging projects into valuable, lasting assets.
Let us help you put the pieces together.
Discover how our expertise can bring structure to your vision.